The Limitations of BMI: What It Doesn't Measure and When It Misleads
BMI is widely used but widely misunderstood. This article explains exactly what the metric can't tell you—and what to use alongside it.
- bmi
- limitations of bmi
- body fat
- health screening
- bmi accuracy
Medical Disclaimer: This article is educational and does not constitute medical advice. Consult a licensed healthcare professional for personalised health assessment.
Body mass index is perhaps the most frequently cited — and most frequently misunderstood — number in medicine. Health agencies use it, employers ask about it, and gym posters quote it. But BMI was designed as a population-level statistical tool in 1832, and applying it to individuals as though it were a precise clinical measurement is a category error that health researchers have been warning about for decades.
This article is not an argument to ignore BMI. The metric has real value when used appropriately. It is an argument for understanding exactly what BMI can and cannot tell you.
What BMI Actually Measures
BMI is calculated by dividing weight (kg) by height squared (m²). It produces a single number that reflects how heavy someone is relative to their height. That is all. It says nothing about:
- The ratio of fat to muscle
- Where body fat is distributed
- Bone density
- Cardiovascular fitness
- Metabolic health markers
When a doctor or researcher uses BMI, they are using it as a proxy for excess body fat — a proxy that works reasonably well at the population level, where individual outliers average out, but that can mislead significantly at the individual level.
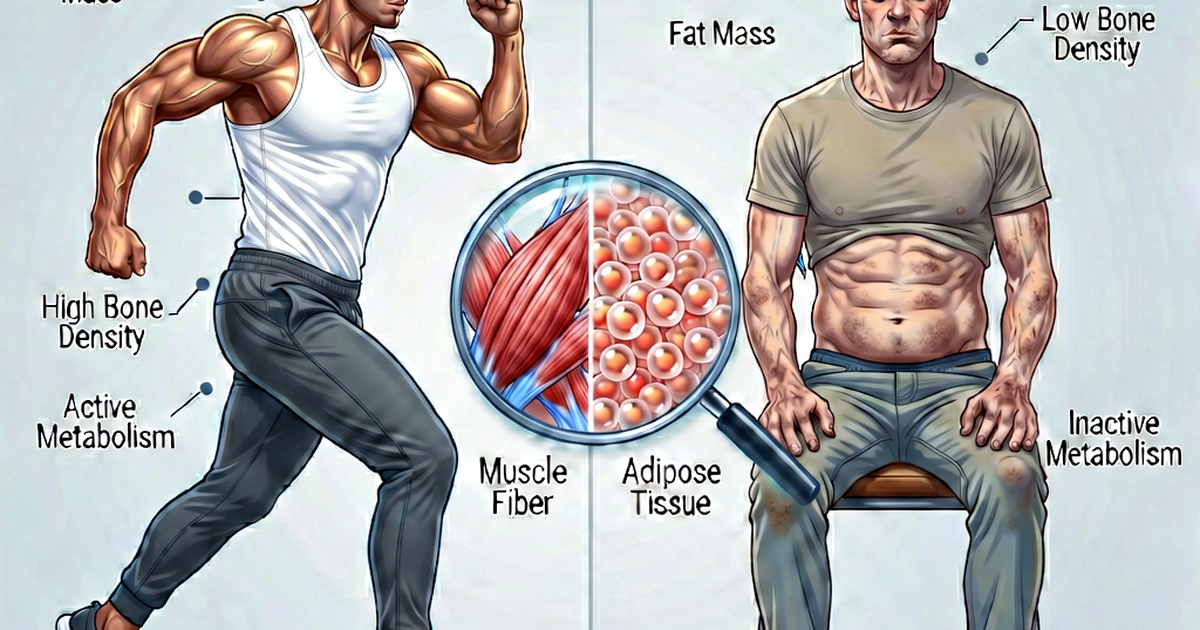
The Muscle Problem
The most commonly cited limitation of BMI is its inability to distinguish muscle mass from fat mass. Both tissue types contribute equally to weight, but metabolically they could not be more different.
Consider: a 5’10” male bodybuilder weighing 220 lbs has a BMI of 31.6, which places him in the Class I Obese category. A sedentary person of the same height and weight, carrying most of that mass as fat, would receive the identical classification. BMI cannot tell these two people apart.
Conversely, someone who has lost significant muscle mass through illness or aging — a condition called sarcopenia — may have a “normal” BMI while carrying a high percentage of body fat. This phenomenon, sometimes called “normal weight obesity” or “skinny fat,” is associated with elevated metabolic risk despite a reassuring BMI number. A 2016 study published in Annals of Internal Medicine found that about 30% of adults with a normal BMI had cardiometabolic risk factors. (Romero-Corral et al., 2010 — Obesity)
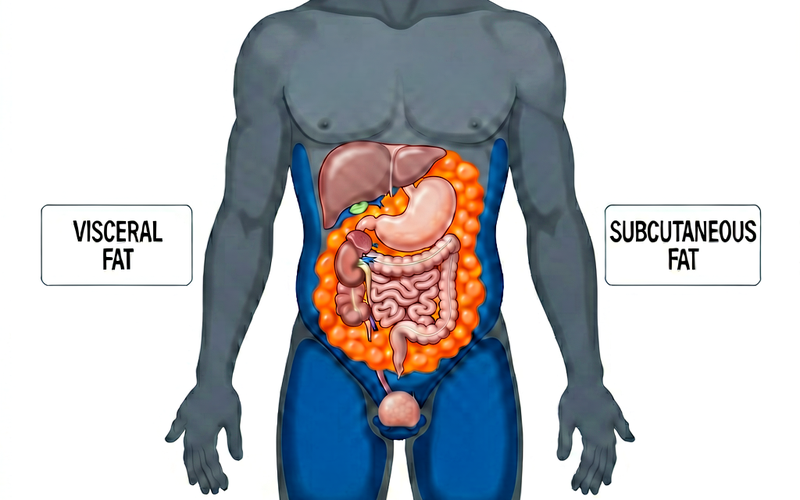
The Fat Distribution Problem
Not all fat is equally harmful. Research has established clearly that visceral fat — fat stored around the abdominal organs — carries substantially higher metabolic and cardiovascular risk than subcutaneous fat stored in the hips, buttocks, and thighs.
Two people with identical BMIs can have entirely different fat distributions and therefore entirely different health risks. This is why waist circumference is increasingly recommended as a companion measure to BMI. The NHLBI recommends that adults with waist circumference above 40 inches (men) or 35 inches (women) are at increased risk, even if their BMI is in the normal range. (NHLBI — Assessing Your Weight and Health Risk)
The Ethnicity Problem
Standard BMI cut-points were derived from studies conducted primarily on populations of European descent. Substantial research since then has shown that these cut-points do not transfer equally across ethnicities.
Asian populations: People of East and South Asian descent develop insulin resistance, type 2 diabetes, and cardiovascular disease at lower BMI values than standard categories suggest. The World Health Organization published a technical report recommending lower action points for Asian populations: public health action at BMI ≥ 23.0, and obesity-equivalent risk beginning at BMI ≥ 27.5 rather than ≥ 30. (WHO — Appropriate BMI for Asian Populations)
Black populations: Some research has found that the relationship between BMI and body fat percentage differs for Black Americans, who on average carry less visceral fat and more lean mass at equivalent BMI values compared to white Americans — which may mean the metabolic risk at any given BMI is somewhat lower. The implications of this for clinical cut-points are still being studied.
The Age Problem
BMI does not adjust for age. At age 25 and age 65, the same person might have nearly identical BMIs despite very different body compositions. The loss of muscle mass that occurs with aging (sarcopenia) is not captured by BMI, yet it is a major driver of frailty and mortality risk in older adults.
Some evidence suggests that in adults over 65, a slightly elevated BMI (25–27) may actually be protective — associated with lower fracture risk and better resilience during acute illness. This “obesity paradox” in older adults is a genuine finding, not an excuse to ignore weight management, but it illustrates that the standard BMI categories were not designed with the elderly in mind. (NIH — Weight and Older Adults)
The Sex Problem
Men and women naturally carry different amounts of body fat at the same BMI. Women typically carry 6–11% more body fat than men at equivalent BMI values, reflecting different hormonal environments and fat storage patterns. The standard BMI categories do not account for this difference.
What to Use Alongside BMI
BMI works best as one data point among several. Clinicians and researchers increasingly recommend combining it with:
- Waist circumference. A simple tape-measure check that captures abdominal fat independently of BMI.
- Waist-to-height ratio. Divide your waist in centimetres by your height in centimetres. A ratio below 0.5 is generally considered healthy; above 0.6 indicates substantially elevated risk.
- Blood lipid panel. HDL, LDL, and triglyceride levels reflect metabolic health more directly than weight does.
- Fasting blood glucose or HbA1c. Insulin resistance and prediabetes can exist at any BMI.
- Blood pressure. Hypertension coexists with obesity but is also common in people with “normal” BMI.
- Body composition testing. DEXA scanning, hydrostatic weighing, or bioelectrical impedance analysis can estimate actual fat mass vs. lean mass — though these methods have their own limitations.
The Bottom Line
BMI is not useless. At the population level it works reasonably well, and for people well outside the normal range in either direction it remains a meaningful signal. If someone has a BMI of 18 or a BMI of 42, that number is conveying real health information.
The danger is treating BMI as a precise individual measure of health or body fatness when it is neither. A BMI in the overweight range does not mean someone is unhealthy. A BMI in the normal range does not mean someone is healthy. The number is a starting point that should be interpreted in context — by a healthcare professional who can consider your full clinical picture.
Use our BMI calculator to find your number. Then take it to your doctor, not the internet.
Related reading
-
What Is a Healthy BMI? Ranges, Categories, and What They Mean
Learn what a healthy BMI range is for adults, how the four official categories work, and why your number is a starting point—not a verdict.
-
BMI vs Body Fat Percentage: Which Is a Better Measure of Health?
BMI and body fat percentage measure different things. Learn when BMI works well, when body fat percentage is more useful, and how to use both to understand your health.
-
BMI Chart for Women: Understanding Your Results by Age and Height
A practical BMI reference chart for women, with height-by-weight tables, age-related context, and guidance on what the numbers mean for your health.